
Jan 25, 2023
A Trauma-Informed Approach Provides Framework for Achieving Health Equity

We have known for years that health equity is possible only through eliminating racism, but we have yet to realize this imperative. The 2021 Future of Nursing Report1 and the Future of Nursing: Campaign for Action2 (an initiative of AARP Foundation, AARP and the Robert Wood Johnson Foundation), the Josiah Macy Jr. Foundation,3 and the American Association of Colleges of Nursing,4 provided key recommendations for health care, including dismantling racism and discrimination. Creating a culture free of racism and focused on equity requires individual and structural changes, and a trauma-informed (TI) approach provides a framework for these changes.
Trauma-informed approaches in health care emerged after the publication of the seminal Adverse Childhood Experiences study (ACEs)5 in 1998. This study highlighted the relationship between experiences of childhood trauma (due to abuse, neglect, and violence), debilitating mental and physical health conditions in adulthood, and early death. The Philadelphia ACEs study in 2013 expanded on the original ACEs by assessing household and community-level exposures to trauma such as witnessing violence, experiencing racism, and living in unsafe neighborhoods, in a diverse and urban sample.6 This landmark study provided evidence of the intersection of race, gender, poverty, and community and the effects of trauma on subsequent risky behavior and poor health outcomes. These studies and evidence from neuroscience research have elucidated the impact of trauma, adversity, and stress on the brain. Understanding changes in the brain as a result of trauma is critical when considering the utilization of services and systems in health care or education, which has often been traumatizing or re-traumatizing, especially for individuals from historically and systemically excluded groups. A TI program, system, or organization realizes the impact of trauma, recognizes signs and symptoms of trauma within oneself and others, responds by making changes to policies, procedures, and practices, and actively resists re-traumatization.7
The TI mindset is as applicable to health care education as it is to health care itself. A TI mindset is defined as acceptance of diversity including background, knowledge, skills, and life experiences; and an understanding that some of those life experiences may be varied and include trauma. Equity-Centered Trauma-Informed Educational Practices (TIEP) adopt the six guiding principles of trauma-informed (TI) care: safety, trust, peer support, collaboration, empowerment, and cultural, historical, and gender issues. The figure below (Figure 1) illustrates an institution or organization’s four phases to becoming trauma-informed.
Figure 1
Equity-Centered Trauma-Informed Educational Practices (TIEP)
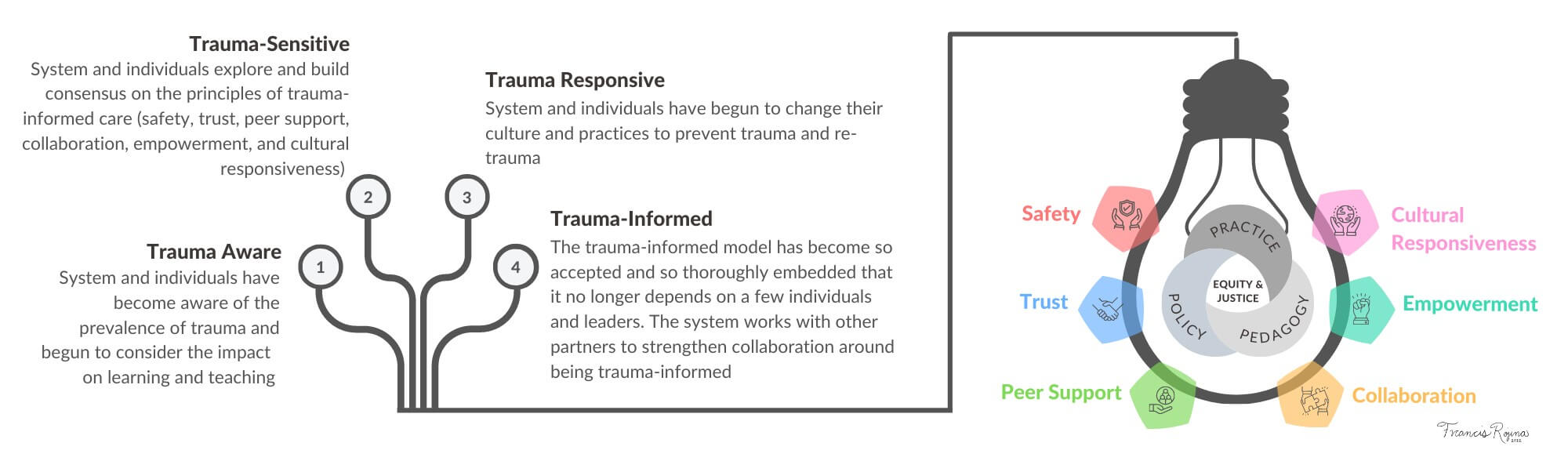
This framework centers on equity and justice, which should be the driving forces behind transforming both health care and health care education. It is important to note that TI is a journey, not a destination, requiring continuous reflection and growth to cultivate a TI lens. The guiding principles should be reflected in the changes we make to practices, pedagogy, procedures, and policies.
In encountering problems with students’ entry or success in our programs, we can apply the TI framework and consider whether our practices breach safety (principle 1) or trust (principle 2). We can look at strategies to enhance peer support (principle 3), collaboration (principle 4), and empowerment through giving voice and choice (principle 5) as ways to achieve equity. Being equity-minded requires an understanding of the cultural, historical, and gender issues (principle 6) that exist as inequities in society are also embedded in our educational environment. For example, recognizing that individuals should not be blamed for their learning gaps, but rather a system that has provided access to education and resources for some while disadvantaging others.
Suppose we believe our society is built on Western values and ideals supporting white superiority. In that case, we must recognize societal inequities permeate systems and structures of higher education and health care. One way this happens is through epistemologically grounded beliefs where ways of knowing and doing have been historically confined to the dominant culture, and many times other cultures silenced and excluded.8–10 If ways of knowing are aligned with white superiority and colonialism, it stands to reason that so do our practices and policies.
In addition to using TI in our educational institutions, we must also work with partners and practicing nurses to strengthen collaboration in utilizing trauma-informed approaches in clinical settings. We must continue to examine ways nursing reinforces societal inequities. Through the TI framework, we can begin to deconstruct historical and cultural oppressions and the role they play in health care and health care education.
Wellness is inextricably linked to the organizational changes called for by a TI framework. Trauma-Informed Oregon11 outlines the reasons TI requires a focus on wellness, including: 1) the role of health care providers and educators can often be difficult and draining; 2) historically and systemically excluded groups have been underpaid, undervalued, and subjected to micro/macro aggressions and discrimination; 3) conditions for health care providers and educators can be stressful (COVID and recent outbreaks of other viruses, such as RSV and influenza, have only intensified these conditions); 4) challenges of being trauma-informed when individuals are experiencing past and/or current toxic stress in the work environment. Audre Lorde says that “caring for myself is not self-indulgence, it’s self-preservation and that is an act of political warfare.”
Equity minded nurses focused on diversity and equity work recognize that promoting inclusion and justice can be lonely and depleting, but TI can refuel and sustain our activism. For others, a TI approach can facilitate the process of becoming equity-minded and calls us to be activists in promoting justice.
TI is about finding our shared humanity, as Van der Kolk12 states:
…[these] fundamental truths; 1) our capacity to destroy one another is matched by our capacity to heal one another. Restoring relationships and community is central to restoring well-being 2) language gives us the power to change ourselves and others by communicating our experiences, helping us to define what we know, and finding a common sense of meaning, 3) we have the ability to regulate our own physiology including some of the so-called involuntary functions of the body and brain through such basic activities as breathing, moving, touching and 4) we can change social conditions to create environments in which children and adults can feel safe and where we can thrive. When we ignore these quintessential dimensions of humanity, we deprive people of ways to heal from trauma and restore their autonomy. Being a patient, rather than a participant in one’s healing process, separates suffering people from their community and alienates them from an inner sense of self.
TI approaches allow us to build interpersonal relationships, cope with new challenges, learn from mistakes, and collaboratively redesign and transform health care and health care education. Being informed is not enough; as equity-minded nurses and educators, we must recognize that we are the drivers of change, and only collectively will we achieve equity and justice.

Rana Najjar is Associate Professor of Nursing at Oregon Health & Science University School of Nursing – Monmouth and leading the work on Equity-Centered Trauma-Informed Education.
References
- National Academies of Sciences, Engineering, and Medicine. The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. National Academies Press; 2021:25982. doi:10.17226/25982
- Campaign for Action. Improving health equity. Future of Nursing: Campaign for Action at the Center to Champion Nursing in America. Accessed November 12, 2022. https://staging.campaignforaction.org/issue/improving-health-equity/
- Humphrey HJ, Levinson D, Nivet MA, Schoenbaum SC. Addressing harmful bias and eliminating discrimination in health professions learning environments: An urgent challenge. Acad Med. 2020;95(12S):S1-S4. doi:10.1097/ACM.0000000000003679
- AACN Statement on Academic Nursing’s Call for Liberty and Justice for All | Elsevier Enhanced Reader. doi:10.1016/j.profnurs.2020.06.009
- Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. Am J Prev Med. 1998;14(4):245-258. doi:10.1016/S0749-3797(98)00017-8
- Cronholm PF, Forke CM, Wade R, et al. Adverse childhood experiences. Am J Prev Med. 2015;49(3):354-361. doi:10.1016/j.amepre.2015.02.001
- Substance Abuse and Mental Health Services Administration (SAMHSA). SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. Substance Abuse and Mental Health Services Administration; 2014. https://ncsacw.acf.hhs.gov/userfiles/files/SAMHSA_Trauma.pdf
- Beard K, Iruka IU, Laraque-Arena D, Murry VM, Rodríguez LJ, Taylor and S. Dismantling systemic racism and advancing health equity throughout research. NAM Perspect. Published online January 10, 2022. doi:10.31478/202201a
- Parson L, Ozaki CC, eds. Teaching and Learning for Social Justice and Equity in Higher Education: Foundations. Springer International Publishing; 2020. doi:10.1007/978-3-030-44939-1
- Cushman E. Decolonizing validity. J Writ Assess. 2016;9(1). Accessed November 15, 2022. https://escholarship.org/uc/item/0xh7v6fb
- Trauma Informed Oregon. Workforce wellness and trauma informed care overview. Trauma Informed Oregon. Published 2022. Accessed December 28, 2021. https://traumainformedoregon.org/wellness/wellness-and-trauma-informed-care/
- Van der Kolk BA. The Body Keeps the Score: Brain, Mind and Body in the Healing of Trauma. Penguin Books; 2015.